I’m always looking for ways to make the most out of my workouts without risking anything else. For instance, I take BCAAs to help repair my muscles after a tough workout. I do not take anabolic steroids to up my performance because those are dangerous. I’m willing to try things that don’t have risks. Because I’m interested in burning the highest amount of calories with the shortest amount of time in the gym, I do short intense workouts to increase my afterburn. Afterburn and creatine are closely related, but the subject is kinda deep. Here we go.
“Afterburn” is an informal name for the science term “exercise post-exercise oxygen consumption” or EPOC. EPOC is the process of taking in oxygen at a higher rate than normal after exercise (1). EPOC occurs with a greater effect after anaerobic exercise. Anaerobic exercise pathways are activated by fast-twitch muscles, which are used for anything intense (2). Prolonged activities that require short energy bursts also activate anaerobic pathways for energy and muscle recovery between bursts (3).
I like my afterburn high. The top line (solid, with squares) represents high-intensity exercise (75%) compared with the others. On the x-axis, the measurement of EPOC starts at 0.
There are two types of anaerobic pathways: anaerobic glycolysis, and high-energy phosphates. The glycolysis pathway uses blood glucose and muscle glycogen stores, with a build-up of lactic acid. Aerobic glycolysis utilizes the same pathway more efficiently when oxygen and ATP are available. Anaerobic glycolysis has a by-product of lactic acid which is what causes the sore, tired feeling in muscles during exercise, but for extremely fast actions like a heavy lift or a jump, anaerobic high-energy phosphate pathways are used (4).
Adenosine triphosphate (ATP) and creatine phosphate (CP) are compounds stored in the muscles. When either is catabolized, a large amount of energy is released. ATP is the energy molecule utilized by most energy pathways, so after one phosphate group is lost by ATP making is ADP (adenosine DIphosphate), CP can donate its phosphate group to ADP becoming creatine, which is a nitrogenous organic acid that many athletes consume as a supplement. The energy released by CP is coupled with the phosphorylation of ADP (5).
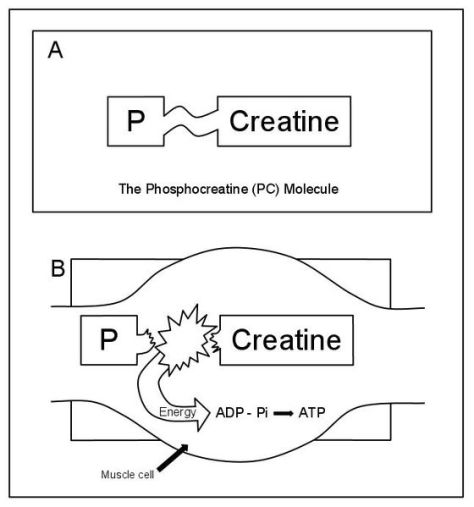
Property of Samuel Tiukuvaara, used with permission
Since only small amounts of ATP and CP can be stored in the muscles, this pathway is used up in under 30 secs (5), but that was published in 1979 before creatine supplements became too popular. Supplements of creatine have been shown to increase the amount of CP stored. During periods of rest, excess ATP can be used to phosphorylate the creatine and supplemental creatine for future energy bursts (6). This is one of the purposes of EPOC.
Think of all that changes physically and chemically during a workout: hormones, fuel stores, cells are damaged, nerves are hyper-aware. The processes required for everything to return to normal require oxygen, hence EPOC (7). ATP and glycogen have been used up, so where does the body acquire another energy source? Fat stores (8). Quite ideal for those of us trying to lose weight. This post-workout fat-burning effect can last anywhere from 3 to 38 hours depending on the exercise intensity and duration (9).
Although aerobic exercise has been found to burn more calories during the workout, anaerobic exercise has a much greater afterburn, and takes energy from the exact place most people want it to: the subcutaneous fat (10). Some of the first studies failed to take calories and diet into account when taking this measurement, but later studies have corrected for this and found similar results (11-13).
Now to me it seems logical that creatine supplementation is somewhat useless considering the muscle cells can only store so much, but being a scientist, I set out to change my own mind. Here are the risks and rewards of creatine supplementation now that you all know what creatine is.
The athletes and fitness gurus who take creatine are usually advised by labels to take a certain amount that contains 2-3x more creatine than would be consumed in a very high protein diet (14). There are many studies claiming risks of creatine dosage, but there is not enough evidence to convince most scientists. The risks caused by creatine supplementation that these studies have claimed are as follows: dehydration and muscle cramping (15, 16), kidney (17) and liver damage (18) in those predisposed , and increased internal production of formaldehyde which is a very damaging chemical (19). One creatine risk that is highly accepted among the scientific community is that creatine supplementation can increase asthma symptoms, even if one does not have asthma (17). Also, many common supplements are laced with heavy metals and toxins. A study conducted by the European Food Safety Authority found that of 33 surveyed products, over 50% had toxic contaminants that exceeded regulation levels (20, 21).
However, there is no truly significant evidence to say that creatine is very dangerous at 5-20 mg/day. Also, it has been shown to increase muscular output in about 70% of studies by increasing the amount of creatine available for phosphorylation before a workout, and de-phosphorylation during a workout (22). A number of athletes have been shown to have increased performance from creatine supplementation, but it is most beneficial for short, higher intensity activities (23). For about 40% of individuals, there is no increase in output because muscles are unable to further store creatine in creatine pools in the muscles (24). Genetics? Yeah, probably the differences in the expression of the gene coding for a creatine transporter. Read more about it here.
This study (25) attempted to bypass the creatine transporter by combining creatine with combinations of other things to no avail. It seems like it will either work for you or not. There isn’t much you can do about it. (PLA = placebo, CRT and CEE are variations of creatine to try to get around the transporter. Notice the plateau for both creatine variations after Day 6)
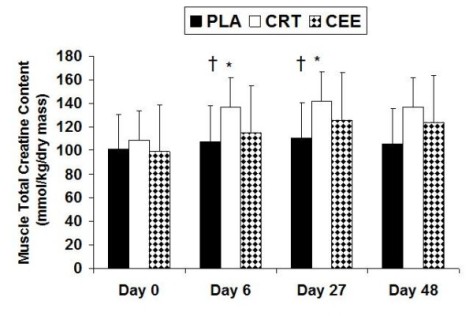
Changes in muscle total creatine with data expressed as mean (± SD). † indicates a significant difference among groups where the PLA group was significantly less than the CRT (p = 0.026) and CEE (p = 0.041) groups.
Spillane et al. Journal of the International Society of Sports Nutrition 2009 6:6 doi:10.1186/1550-2783-6-6
There is sound evidence here that regular creatine supplementation can increase athletic performance for some, 60-70% of people. Some studies claim that creatine increases muscle mass, but there is no sound evidence for that claim. Creatine increases energy expenditure. It does not directly affect muscle mass, in my opinion. This idea that it can is probably an indirect assumption stemming from increasing exercise which increases muscle damage which THEN increases muscle mass by incorporating protein and glycogen into healing the muscles, making them bigger.
There is also a claim that if weight loss is you goal, avoid creatine. There is no sound evidence for this, but it makes sense to me this way. I want a great big afterburn every time I work out. I want to be losing/maintaining my weight when I’ve been out of the gym for 12 hours. The purpose of creatine is to speed the recovery and avoid dipping into other energy sources like fat stores. I WANT to get into those fat stores. What I have just said has no scientific backing, but many have complained about not losing weight when supplementing with creatine.
If your goal is only performance, go for it with caution. If you want to lose weight, my gut says avoid it. I’m a fan of going as natural as possible. If it weren’t for the scary contaminants that have been found in a lot of creatine, I might have given it a try.
I welcome anyone’s opinion on this topic, as I could be totally wrong about losing the afterburn.
1. Scott CB, Kemp RB (January 2005). “Direct and indirect calorimetry of lactate oxidation: implications for whole-body energy expenditure”. Journal of Sports Sciences 23 (1): 15–9.
2. Medbo, JI; Mohn, Tabata, Bahr, Vaage, Sejersted (January 1988). “Anaerobic capacity determined by maximal accumulated O2 deficit”. Journal of Applied Physiology 64 (1): 50–60. Retrieved 14 May 2011.
3. Scott, Christopher B (June 2005). “Contribution of anaerobic energy expenditure to whole body thermogenesis”. Nutrition & Metabolism. 14 2. doi:10.1186/1743-7075-2-14. Retrieved 14 May 2011.
4. Di Prompero, PE; G. Ferretti (Dec. 1). “The energetics of anaerobic muscle metabolism”.Respiration Physiology 118 (2-3): 103–115.
5. Fox, Edward (1979). Sports Physiology. United States of America: Saunders College Publishing. pp. 9–11
6. Schlattner, U.; Tokarska-Schlattner, M., and Wallimann, T. (2006). “Mitochondrial creatine kinase in human health and disease”. Biochimica et Biophysica Acta – Molecular Basis of Disease 1762 (2): 164–180
7. Saladin, Kenneth (2012). Anatomy & Physiology: The Unity of Form and Function. New York: McGraw Hill. p. 425.
8. Bahr R (1992). “Excess postexercise oxygen consumption–magnitude, mechanisms and practical implications”. Acta Physiologica Scandinavica. Supplementum 605: 1–70
9. Schuenke MD, Mikat RP, McBride JM (March 2002). “Effect of an acute period of resistance exercise on excess post-exercise oxygen consumption: implications for body mass management”. European Journal of Applied Physiology 86(5): 411–7.
10. “Impact of Exercise Intensity on Body Fatness and Skeletal Muscle Metabolism”. Exrx.net. Retrieved 2010-07-29.
11. Reynolds, Jeff M; Kravitz, Len. “Resistance Training and EPOC”. Retrieved April 21, 2005.
12. Børsheim E, Bahr R (2003). “Effect of exercise intensity, duration and mode on post-exercise oxygen consumption”.Sports Medicine 33 (14): 1037–60.
13. Baker, E. J., and T. T. Gleeson. EPOC and the energetics of brief locomotor activity in Mus domesticus. J. Exp. Zool. 280: 114–120, 1998.
14. “Creatine – Sources in the Diet”. Examine.com. Retrieved 22 January 2013.
15. Lopez RM, Casa DJ, McDermott BP, Ganio MS, Armstrong LE, Maresh CM (2009). “Does Creatine Supplementation Hinder Exercise Heat Tolerance or Hydration Status? A Systematic Review With Meta-Analyses”. Journal of Athletic Training 44 (2): 215–23.
16. Dalbo VJ, Roberts MD, Stout JR, Kerksick CM (July 2008). “Putting to rest the myth of creatine supplementation leading to muscle cramps and dehydration”. British Journal of Sports Medicine 42 (7): 567–73.
17. “Creatine: Safety”. MayoClinic.com. Retrieved 2010-08-16.
18. Poortmans JR, Francaux M (September 2000). “Adverse effects of creatine supplementation: fact or fiction?”. Sports Medicine 30 (3): 155–70.
19. Francaux M, Poortmans JR (December 2006). “Side effects of creatine supplementation in athletes”. International Journal of Sports Physiology and Performance 1 (4): 311–23.
20. Moreta S, Prevarin A, Tubaro F. (June 2011). “Levels of creatine, organic contaminants and heavy metals in creatine dietary supplements”. Food Chemistry 126 (3): 1232–1238.
21. Pischel I, Gastner T. (2007) Creatine – its chemical synthesis, chemistry, and legal status. Subcell Biochem 46:291-307
22. Bizzarini E, De Angelis L (December 2004). “Is the use of oral creatine supplementation safe?”. The Journal of Sports Medicine and Physical Fitness 44 (4): 411–6.
23. Kerksick C, Harvey T, Stout J, Campbell B, Wilborn C, Kreider R, Kalman D, Ziegenfuss T, Lopez H, Landis J, Ivy JL, Antonio J (2008) International Society of Sports Nutrition position stand: nutrient timing. J Int Soc Sports Nutr 5:17 (Erratum in J Int Soc Sports Nutr 5:18)
24. Kreider R: Creatine supplementation: analysis of ergogenic value, medical safety, and concerns. JEPonline 1998, 1:1-6
25. Spillane, M; Schoch, R; Cooke, M; Harvey, T; Greenwood, M; Kreider, R; Willoughby, DS. “The effects of creatine ethyl ester supplementation combined with heavy resistance training on body composition, muscle performance, and serum and muscle creatine levels”. Journal of the International Society of Sports Nutrition 6: 6










